Service planning and responding to proposed changes
Information to help you plan your service
You may also want to view our pages on Workforce planning, staffing and resources
Last updated: February 2026
 Download as PDF
Download as PDF- Introduction
- Considerations for service planning
- Process for planning speech and language therapy services
- STEP 1: Assessing the needs of the local population
- STEP 2. Analyse the current speech and language therapy service
- STEP 3. Review and design service options
- STEP 4. Preparation for your business case
- Responding to planned changes to your service
- Influencing decision makers
- Responding to proposed changes to terms and conditions of employment
- National guidance and legislation
- Resources
- Contributors
Introduction
Services need to be planned, taking into account national policies and guidelines, current evidence-based practice and research findings, and expert opinion as well as service user consultation and co-production within the local context. Here you will find information that should help you plan your service. Support for service managers and clinicians in responding to proposed changes to service provision will also be explored throughout this guidance.
Considerations for service planning
When planning services, speech and language therapy service managers and leaders should take account of the relevant key points in multidisciplinary/ integrated care pathways where speech and language therapy services are essential or beneficial.
Services need to be planned taking into account:
- national policies and guidelines including HCPC standards; Clinical guidance A to Z for national guidance on specific topics; RCSLT guidance to support members to meet the HCPC standards
- current evidence-based practice/research findings: Please see research and clinical guidance A to Z for national guidance on specific topics
- expert opinions of clinical leaders, providers and service users. Stakeholder and service users should be involved when assessing the needs of the local population and in considering service redesign options. Service user consultation and co-production should be considered within the context of partnership working (with colleagues in health, education, social care and voluntary services) across local integrated care systems
- current service activity data and outcomes. Please see Monitoring, audit and evaluation; Outcome measurement ; Quality services and quality improvement for more information
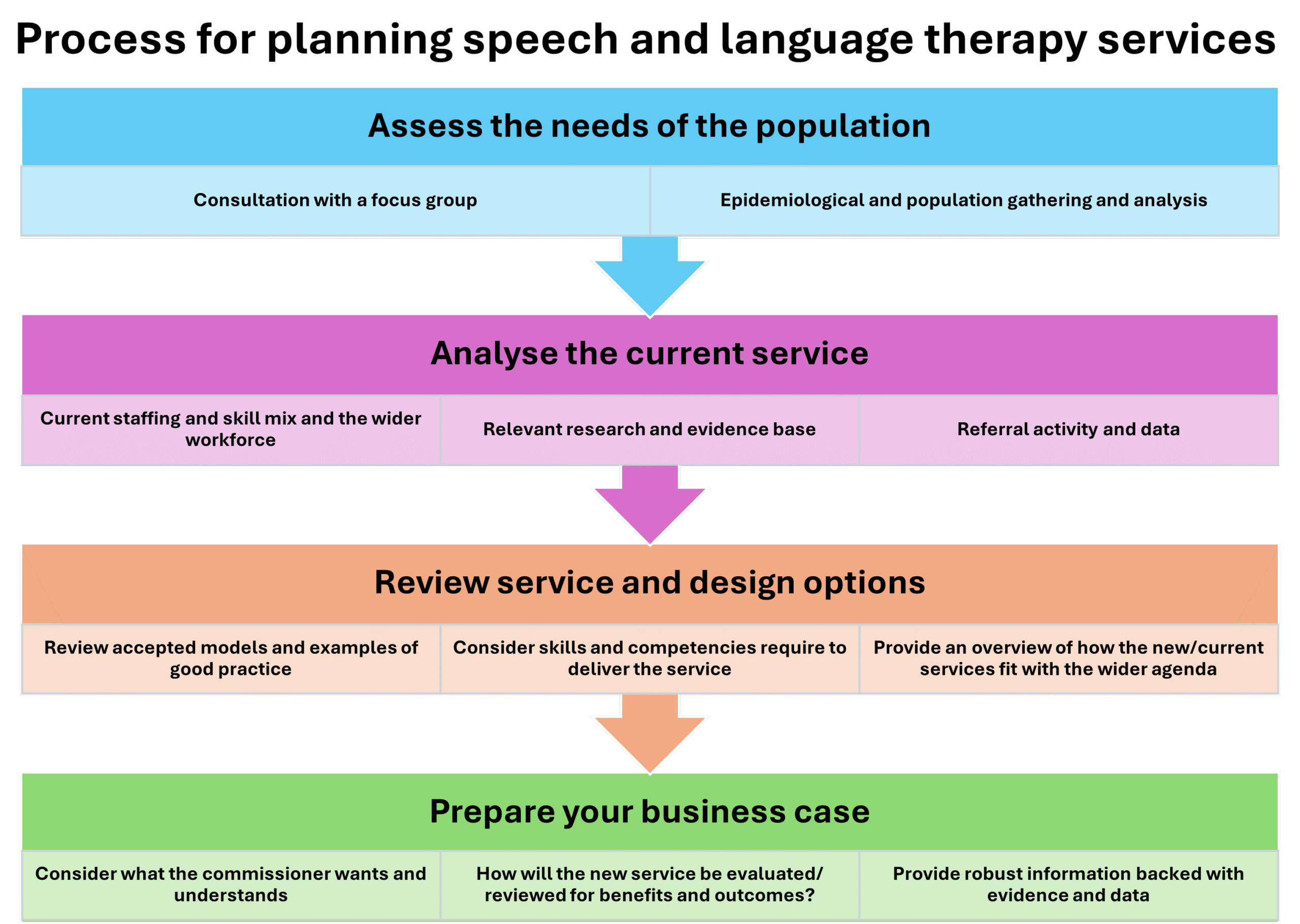
Process for planning speech and language therapy services
There are four key steps to for planning services:
- assessing the needs of the population
- analysing the current speech and language therapy service provision
- reviewing design models of service delivery that can meet the population needs
- preparing your business case.
This methodology will be useful in reviewing current services and in planning for service developments.
STEP 1: Assessing the needs of the local population
Understanding the needs of a local population supports equitable, evidence based, accessible, relevant and efficient services. See RCSLT health inequalities pages for further information on this topic.
Why carry out a local needs assessment?
- To ensure that speech and language therapy services are providing a range of secondary and tertiary-level services to appropriately meet local communication, eating, drinking and swallowing needs.
- To inform the process of identifying local health and wellbeing needs, education and social needs.
- To highlight to commissioners the needs and impact of potential communication and eating/drinking and swallowing difficulties within: care groups; care pathways and within wider population groups.
When services are operating with insufficient resources to meet demand, an annual needs assessment of the service-wide population should be carried out and linked to an analysis of effectiveness, to ensure that resources continue to be allocated to the most appropriate areas of service. A re-evaluation of the services currently provided in terms of skill mix, is also recommended.
How to carry out a local needs assessment
In undertaking a local needs assessment for speech and language therapy service development there are several processes that can be employed:
- Consultations with commissioners, service users, referral agents and co-providers of services to assess levels of satisfaction
- Health/population intelligence estimating current unmet need using epidemiological and population demographic analysis
- Service level data relating to provision, outcomes, demand/unmet need for this population.
Consultations
Bids for service development need to link in with local planning processes and priorities. It is advisable to alert commissioners and other stakeholders to the need for in-depth service evaluation at an early stage of development. This process will enable you to identify local drivers and priorities of commissioners and partners. Your stakeholder analysis should help you to identify key groups to consult.
Consultation with local clinical leaders
When reviewing a service for a specific population or group, seek the views and inputs of clinical leaders (including Speech and Language Therapists) at an early stage. Their support with service changes and development bids proposals will be essential to a smooth process.
Consultation with partners
As most speech and language therapy services are not provided in professional isolation, most plans for service development require the involvement and cooperation of other people.
SLT’s may wish to explore funding opportunities with charities, Local Authorities, neighbourhood developments and HEI’s as development bids which are able to demonstrate partnership working and integration across the system, internally or externally, may increase the likelihood of a successful development bid.
Consultation with other services should include discussion related to current integrated care pathways, the roles, functions and skills of the current staff and those required of the future workforce.
Consultation with service-users
In the context of the patient-led NHS agenda, information based on need and demand linked to an analysis of effectiveness and efficiency is particularly powerful and persuasive. Try to capture as much information from service-users as possible. For example, if a language unit is to be added to a local school, you should consult with the speech and language therapy service-users attending the school and their parents. Aim to be as comprehensive as possible in your survey and include the school authorities, teachers and assistants working in the school as well as the local education department, referring educational psychologists and other health professionals working within that school’s catchment area.
To look at a larger development, you may need to consult with a sample of services, both of users and other professionals, with whom you can collaborate. For example, to review a paediatric speech and language therapy service, you could survey a representative sample, using results taken from each of the locations that children’s services are provided in, without having to conduct research with every user, parent and member of staff at that location.
These samples should be based on a fair representation of the demographic and population variables that exist. By ensuring samples are taken addressing the full range of demographic variables, you will be able to extrapolate from the data/results information on services/locations that you have not been able to look at directly in your research. From this extrapolation, you should be able to derive a picture of the competencies and workforce numbers required for your service (or at that location) as a whole.
You may want to carry out these consultations through face-to-face contact with individuals, small or large groups and with separate or mixed audiences. When deciding which method or methods you employ, you should consider the scale of the consultation required, the relative importance of the audiences you are consulting with and, of course, your capacity to fund and carry out the consultative work.
At the start of every consultation, you should explain the purpose of the consultation, perhaps though giving a short presentation explaining what speech and language therapy is about and the different models of service delivery that are under consideration. It might help you to record or video your contact with important audiences (with their permission, of course), as this may help to facilitate accurate analysis of the views expressed and themes that may emerge.
Examples of locations where you might carry out consultations:
- education settings
- primary and/or secondary schools
- special schools
- specialist units
- nurseries
- health settings
- hospitals
- community clinics
- residential settings
- care homes
- residential homes
- nursing homes
- prison.
Health/population intelligence
Using epidemiological and population demographic analysis will inform service managers on areas of need and can be used to support targeting resources and priority setting within and across services. The tool kits listed below are sources of health and population intelligence. You could also contact local public health colleagues, health economists in NHS trusts or other Local authority or health leads who may have access to local data sets.
UK-wide
- Local statistics from the Office for National Statistics (ONS).
- National statistics– official statistics produced impartially and free from government influence.
England
- Health profiles England– provides a snapshot of health statistics across England. Can assist local needs assessments, policy, planning and performance management.
- Fingertips – a large public health data collection, data organised into themed profiles for example child and maternal health.
- National child and maternal health intelligence network– provides child and maternal health statistics, which aim to improve decision-making when planning services for children, young people and mothers.
- Information provided by Gov.uk
- Royal College of Physicians’ Sentinel Stroke National Audit Programme
Scotland
- Public health information service for Scotland– provides interactive graphs and reports for health and wellbeing in local areas across Scotland.
- Scotland’s official statistics with over 250 datasets from a range of producers.
- Census– this includes questions on disabilities and lifelong conditions which may be useful to assist your case
Wales
- Statistics and research– major independent source for current and historical releases of official statistics and social and economic research on Wales.
- Stats Wales – detailed official data on Wales.
- Official statistics from Public Health Wales.
Northern Ireland
- Public Health Northern Ireland
- Northern Ireland Statistics and Research Agency(NISRA) – provides a range of statistics for Northern Ireland, including for population.
- Health inequalities statistics from the Northern Ireland health and social care inequalities monitoring system (HSCIMS).
- NISRA census
STEP 2. Analyse the current speech and language therapy service
Analysing a speech and language therapy service requires consideration of
- current staffing levels and the mixture of skills, specialities and experience among speech and language therapy services and the wider workforce
- referral and activity data, including data that is relevant to service demands and capacity to deliver services
- relevant outcome data for each element of the service (see RCSLT Outcomes Measurement)
- models of speech and language therapy service delivery.
Method for assessing current skill mix and establishment
- Conduct an audit of the speech and language therapy service’s current staffing levels and skill mix. Information on the effect of these numbers for proposed service developments and how skill mix, resources and demographics influence can be found on the Workforce planning, staffing and resources page.
- The audit should highlight the benefits and risks of the current service model and how the service is currently mitigating any risks, which includes raising these issues with service commissioners and other relevant partners. Risks identified during this assessment should be recorded on your employer’s risk register as indicated.
- Analyse the staffing levels and the current skill mix for all professional and allied staff groups within the selected educational, residential and health settings where the service operates. Ask local authorities to provide the relevant staffing figures for those settings or ask them for assistance with requesting the information from the relevant heads of service.
- It should be possible for you to produce a comprehensive staffing profile of the speech and language therapy skill mix the service and administrative staff requires for each type of setting by looking at: the available skill mix; the functions that must be carried out (outputs and outcomes) and staff competencies required; the population information; the current caseload; the number and mix of locations in which the service is to be delivered; the model of practice chosen.
This information will support heads of service in planning and costing changes to their skill mix for service delivery redesign. It also provides a concise depiction of costed skill mix change proposals.
Don’t forget! As part of assessing the required staffing establishment, planned time off for annual leave and study for continued professional development must be taken into account as well as allowing time for possible unplanned leave to cover illness, parental responsibilities or compassionate leave. Taking this into account, for every whole-time equivalent therapist funded for approximately 52 weeks of the year, around 42 weeks are available for work.
See NHS England AHP job plans. And RCSLT Staffing and Resources
Accommodation and other resource requirements
Potential non-staff costings involved in running/setting up proposed service should be included in analysis and business proposals.
This may include:
- access to appropriate accommodation to deliver safe and effective service which complies equality, diversity and inclusion/belonging legislation. Service leads should identify specific accommodation requirements in relation to proposed service offer to create communication-friendly environments for both clinical and administrative functions including rental, running costs and furnishings. See RCSLT guidance on inclusive communication
- costings for specialist assessments and equipment required to deliver clinical services including any staff uniform required where this is supplied by the service
- subscriptions to accessing digital systems to work with service users, hold video conferencing style meetings or for clinical and service management (e.g. storing electronic patient records, service activities and reporting)
- any organisational overheads needed, such as a contribution to central teams i.e. finance, human resources, IT, etc
- staff travel and training costs based on current levels of expenditure and the anticipated models of working.
Recurrent costs should be set out separately from any non-recurrent costs (for example start-up costs i.e. new laptops for additional staff, one off purchases etc).
Method of analysing current speech and language therapy activity
One of the best ways to demonstrate the value of a service is to collect relevant information and data sets. Commissioners and others want to know about quantitative and qualitative measures of the success and impact of a service. Data collection and audit should be an ongoing process and embedded within local clinical governance frame works. Dedicate time to identify the information that is required for service management purposes and to determine any additional information stakeholders will require.
The cooperation of the entire team will be needed to collect the correct data. The team will need to understand why the data is required and what it will tell others about the service. There needs to be a shared understanding that data must be robust, consistent, accurate and provided on time, so that the correct information about the service is available when needed.
Set aside time to provide feedback to individual staff members and the team as a whole.
Qualitative measures
Qualitative measures describe outcomes against national and local priorities. They provide context for decision-makers that can help illustrate the value of a service. Information on caseloads, standards and evidence on the effectiveness of speech and language therapy is available through the RCSLT’s clinical guidance pages.
You may find it useful to refer to these sources of evidence when developing a picture of how speech and language therapy adds value to other health and social care activities.
Qualitative information from patients
Patient and public involvement, engagement and participation are at the centre of current Government thinking on the provision of health care services. Patient satisfaction and feedback provide important evidence as about how well a service is delivering care.
Patient, parent or carer focus groups can be very useful tools to help gather detailed, qualitative information on public expectations for speech and language therapy. Additionally, patient surveys, complaints and compliments received are also useful sources of information. See information on consultations.
Other qualitative measures
Qualitative measures might also include endorsements from other NHS staff (for example, ENT surgery teams, stroke teams, paediatric teams, GPs) or other professionals involved with your patients (health workers, teachers, prison and probation officers, social workers).
Multidisciplinary teams and integrated care pathways
It is important to demonstrate how a service fits in with other healthcare, social care and education teams in delivering integrated care to local populations: how it contributes to population health preventing illness, tackling health inequalities; and how it contributes to national and local priorities (i.e. NHS long term plan, SEND agenda for 0-25 year olds).
Quantitative measures
Collecting and analysing quantifiable data from past service activity will assist your planning and redesign. The table below outlines data sets which you may wish to consider depending upon service area you are reviewing/planning.
| Demographic and epidemiological data | See Step 3 local needs assessment
|
| Satisfaction and Experience Surveys | See Qualitative measures |
| Service Activity and caseload data including service efficiency metrics |
|
| Digital and assistive Technology Use metrics |
|
| Outcome measures |
|
| Benchmarking and Audit data |
|
| Workforce and capacity data | See Workforce planning, staffing and resources
|
| Service Cost and resource used | Relevant financial and resource data for example
|
Electronic record and data collection, such as system 1, EMIS and RiO have made it easier and efficient to pull this type of data. Contact your IT and audit departments for support on how to do this. Your Finance department may be able to support you with analysis and costings for services.
Commissioners of services and workforce planners are interested not just in patient related activity, but in outcomes of interventions and the likely impact both of therapy either being available or not available.
Linking benefits and activity data to the targets and priorities of local agencies will assist with development bids. Information on local targets and priority areas is available from a variety of sources such as national policies and local agency improvement plans.
Demand and capacity
The mismatch between demand and capacity is viewed as one of the main reasons for waiting lists or back logs developing and subsequent waiting times increasing within the NHS. Demand and capacity modelling is viewed as essential by NHS for delivering healthcare services within a modern health and social care system. Demand and capacity modelling can help delivering quality care for patients by showing how different providers and sectors within an integrated care system / local partnership can best work together to deliver services for patients within a locality. It can also ensure that any services provided have enough core capacity to see patients in a timely manner.
A speech and language therapy service or department that is being reviewed may not currently be able to offer the quality or scope of service that you or your clients think is appropriate. Demand and capacity modelling can use data to illustrate to commissioners and others where there are gaps in the service and how they might be addressed. For example, an estimate of the unmet need of a client group or population group can be made by comparing actual referral rates with predicted referral rates (based on incidence/prevalence figures related to population figures).
The NHS England demand and capacity resource gives further insights in to demand and capacity models and tools:
Care should be exercised in using some information as, for example, waiting list numbers and numbers of new referrals may simply reflect local patterns due to the presence or absence of specialists, multi-disciplinary teams, or a particular model of service rather than reflecting actual need. Additionally, the incidence or prevalence rates do not indicate the numbers of people who may benefit from or want speech and language therapy input.
Triage assessment also allows services to profile the unmet need within any waiting lists for therapeutic care. This information can then be used to put forward a case for service development. See screening and referrals in Care Pathways.
Where an analysis of unmet need reveals that the safety of individuals is being put at risk or the efficacy of therapeutic input is seriously compromised, consideration must be given by the speech and language therapy manager to mitigating risks by redesigning the model of service delivery, capping the caseload or withdrawing a service until further support can be achieved. See safeguarding.
STEP 3. Review and design service options
Ongoing service review and the redesign of services facilitates modernisation, improvement, relevance, effectiveness and efficiency of services.
Managers are advised to:
- use best-practice clinical guidance in designing service options and to show how the predicted benefits and outcomes from the service change will be evidenced.
- consider the skills and competencies required to deliver the models in the context of the multidisciplinary/integrated care pathways within which the service is to be delivered.
- design options for models of service delivery that can be provided, including an overview of the staffing establishment, skill-mix of staff and any other associated resources which may be required.
- agreed the processes that need to be undertaken in the context of a multi-disciplinary or multiagency forum with commissioners.
Developing service options requires:
- an understanding of local and national drivers, priorities and strategies
- consideration of local needs and availability of resources
- consideration of risks and safety of service users and staff and mitigations in place
- understanding of the evidence base
- the ability to evaluate the current, and predicted future, service provision and outcomes.
Having identified the need for service development and having clarified the desired outcomes and benefits of such a development, a range of service provision options should be explored. Refer to the steps for planning developing models of service provision and responding to proposed changes to a service for further information.
Predicting future demand requires consideration of local need and national strategies and priorities. Consider current socio-economic and political priorities. What is being promoted as a driver for change and how can proposed service developments tie in with this?
Refer to:
- the relevant employer’s development strategy
- local health provider websites
- local council websites
- relevant charities or lobby groups
- the Council for disabled children
- Government websites e.g. NHS England, Kings Fund, DfE
- statistical information see the ‘health/population intelligence’ section of this guidance.
Collate current service information for use as evidence for future demand – see ‘method of analysing current speech and language therapy activity’ section of this guidance.
This information will help the analysis of present and future demands, such as possible access issues, or the likelihood of long-term and age-related conditions.
Examples of predictors for change include:
- an increasing number of adults and children/babies surviving with disabilities due to technological and medical advances
- the use of technology to provide remote access to impairment therapy
- increasingly affordable and flexible technology to assist individuals with their communication
- Current Government legislation and strategies (or those in development) which are relevant to clinical practice
Keeping up to date with policy developments across the nations
RCSLT’s policy and public affairs team provide briefing documents on a wide range of legislation and policy covering all four UK nations.
If you know what is going on in the wider political and economic fields, you’ll be better prepared for change and better able to respond in the interests of your service-users. See the policy and influencing section of the website for further information.
Considering models of service provision
When developing a model for service provision, service managers should consider the aspects of service found in in Table 1.
Aspect of service model |
Consider |
RCSLT resource |
| Best practice standards |
|
|
| Functions of the proposed service |
|
|
| Competencies required to deliver proposed functions |
|
|
| Staffing skill mix required |
|
|
| Other resources required |
|
|
| Cost implications |
|
|
Service development methodology
Please refer to ‘process for planning speech and language therapy services’ section and ‘staffing and resourcing’ section of ‘workforce planning, staffing and resources’ page (link to be added) to help build a robust case for service developments.
STEP 4. Preparation for your business case
A business case should clearly explain to budget-holders and decision-makers the value and benefits of the proposed service development. By following the steps 1-3 outlined in planning your service, service planners will be ready to prepare a business case. Business cases may be subject to a thorough appraisal process and must answer all questions and concerns a busy organisation may have. It is important that this process and its various stages are understood and whether a particular format/proforma is required before starting to build a business case.
Core components of a business case may include making the case for change; articulating value for money; commercial viability; affordability; and a capability to deliver.
Approval of a business case will involve multiple stakeholders. Revisiting any stakeholder analysis that has been made will help identify relevant stakeholders and what information they will be interested in. Do not assume that decision makers will understand what speech and language therapy is or its impacts. You will need to be ready to explain the value the service brings.
Decision makers will want to know:
- why is this proposed change necessary
- what they are getting for ‘their’ money
- how speech and language therapy services will help to deliver against their priorities
- how speech and language therapy services will help them to achieve financial balance.
It is important to explain the outcomes that can be achieved, how they can be reached, what the impact will be and what success looks like. Stakeholders will want to understand both quantitative and qualitative measures and data sets and it is important that you develop clear and strong descriptions of both.
Key points to include in a business case
- The case for change – outlining the nature of the problem, how this has been identified and explaining how the proposal will address it. Consider an options appraisal where necessary, including risks and benefits of each option. The proposal should address benefits for both service users and commissioners and describe how both groups will benefit from implementing these ideas in terms of efficacy, safety, and any financial benefits identified.
- A clear, succinct description of the service proposed, including demographics, location, patient benefits, resources and staff base.
- A description of how the proposal fits with current service-level agreements.
- Service-user stories – case studies are a powerful way of illustrating the difference speech and language therapy services make to people’s lives.
- Highlight the service’s current and or the proposed service’s unique selling point, including any efficiency savings that would be made.
- Where applicable, show how the service is working in new and innovative ways to improve individual outcomes.
- Where applicable, include details of the risks of not providing speech and language therapy to people with communication eating, drinking and swallowing needs and a ‘doing nothing’ scenario.
- Identify any other risks to success of the proposal and how they can be mitigated.
- Consider drawing comparisons with national standards or local competitors – detailing how a service compares favourably in terms of outcomes, skill base, cost effectiveness.
- Give information on staff (SLTs, assistants, administrative support), and non-staff costs (equipment, accommodation, finance, HR and governance/management systems).
- Describe how the service will be monitored and evaluated.
Responding to planned changes to your service
Ongoing service review and redesign can facilitate modernisation, improvement, relevance and efficiency of services and can have positive impacts for service users and service providers. However, there are occasions when concerns are raised that proposed changes to your service’s structures and priorities could lead to:
- a risk to the safety of service – users or SLT staff
- the service provided would be detrimental to or of no benefit to service-users
- the service provided or not provided would breach your duty-of-care
- the service provided or not provided would expose you to risk of referral to the Health and Care Professions Council.
It is in service users’ best interests for managers and professional leads to proactively identify the information their audience groups need to know. A stakeholder analysis may help identify key individuals or groups who can influence the decision making and what information to collect. Budget holders and decision makers, for example, may be focused on how many patients’ individual therapists are working with. It is essential that they are provided with details of direct and indirect activity, to help them understand the diverse range of functions which SLTs carry and their contribution to patient pathways. They will also need to understand the benefits of speech and language therapy to patients and communities. Managers and professional leads will have to explain the risks and impacts of not providing some services, presenting evidence and data to support their case.
It is important to bear in mind service demands, pressures to improve patient outcomes, productivity and value for money are being felt across the whole health care system and not just speech and language therapy services. In explaining the benefits of speech and language therapy, managers will need to highlight where services contribute to national and local priorities.
Further help
If you require any further advice, please contact RCSLT on info@rcslt.org.
Influencing decision makers
The right information, data and evidence is key to influencing commissioning and stakeholders. When collecting and analysing local data, consider and include:
- direct and indirect services
- client attributable and whole systems activity
- service development and organisational development activities
- relevant feedback from service users and stakeholders on outcome and impact of the service.
This will help to explain what services are provided and why, see ‘Process for planning speech and language therapy services’ on this page for associated reading.
Link output to outcomes
Illustrate the effectiveness of the service by using qualitative data. For more information see: Outcome measurement, Monitoring, audit and evaluation.
Use local and national benchmarks
Make comparisons against recognised standards see ‘Step 3 Review and designing service options’.
Education: Through demonstrating how speech and language therapy makes a difference to people’s lives, planning services helps educate commissioners and stakeholders by providing them with answers to their questions as well as answering questions they may not have thought to ask in the process.
Managing funding cuts
Financial savings targets and cuts are a reality for many managers as organisations drive to improve efficiencies in health services. A clear and proactive response is required to maintain effective, efficient and qualitative services.
Holding an options appraisal, taking risk assessments and considering the skill mix of a service will help manage any response to funding cuts.
Options appraisal
Defining how a service might be reconfigured will enable budget-holders and decision-makers to take a view on how services can help to address local priorities. Depending upon the service area these decision makers maybe external to health services i.e. local authorities, third sector or schools.
Others may not see speech and language therapy services as fitting neatly with ‘health provision’. Refer to national and local drivers to illustrate how a service contributes to addressing local and national health priorities. Help budget-holders and decision-makers to make difficult decisions in an informed manner by providing them with clear options evidence base, including associated risks and mitigations.
Remember that each service contributes to other care pathways, which might also be affected by cutbacks. If a cutback is being proposed, highlight the consequences for the service and its ongoing ability to meet local priorities. Address the immediate and longer-term effects on patient health and future increases in care costs as set out in the rest of this guidance.
Risk assessment
To identify the benefits, value and impact of speech and language therapy to patients and communities, managers/professional leads will need to explain the risks/impacts of not providing some services, presenting evidence and data to support their case.
A risk assessment should be used to illustrate what will happen if a service is cut back. This can be a very persuasive and informative tool that help communicate the value of speech and language therapy services to commissioners and others. Link identified risk back to any legislation/statutory functions which might be breached if cuts are implemented and the impact for organisations concerned
A pre-existing service will have gathered evidence through its activities (particularly from quantitative measures) that will demonstrate the impact of cutting staff and/or budgets for its clients and patients. Draw attention to this impact on services and illustrate it with evidence. Qualitative evidence regarding patient outcomes, potential impacts on other services i.e. relationship between SLCN and mental health services can also be used to achieve this.
See the resources and references section of this guidance for further useful information.
Responding to proposed changes to terms and conditions of employment
If proposed changes to a service include changes to any employee’s terms and conditions of employment, we recommend that employees approach their trade union in the first instance. Employees may also wish to consider contacting their human resources department, Chief AHP/Executive Director of AHP’s or their Trusts’ ‘Freedom to Speak Up Guardians (FTSUGs)’ if working for the NHS.
As the professional body for speech and language therapy, RCSLT is not able to help with employment-related problems.
Unite is the trade union which represents most speech and language therapists. It provides free legal advice and representation to members who have employment-related problems.
National guidance and legislation
Equity, diversity and belonging
- RCSLT has an Equity, Diversity and Belonging Vision to build a profession where every voice is valued, every identity respected, and every practitioner empowered to thrive
- The UK Equality Act (2010) legally protects people from discrimination in the workplace and in wider society. It includes many of the provisions in the UK Disability Discrimination Act (1995) which makes it unlawful to discriminate against disabled people in areas like employment and access to services.
- Health and safety legislation
- Health and Safety Executive provides guidance on health and safety. Failures to implement or to inform staff about health and safety policies can affect duty of care.
- Public interest disclosure – Public Interest Disclosure Act 1998 protects employees who ‘blow the whistle’.
- Public Concern at Work – whistle blowing commission which was founded by public concern at work and can provide more information and has a helpline.
- Freedom To speak up – Freedom to Speak Up Guardians support workers to speak up when they feel that they are unable to do so by other routes. They also work proactively to support their organisation to tackle barriers to speaking up. Their role is independent and impartial.
- Equality and Human Rights commission provides guidance on the implications of equality legislation and working time regulations. Their website provides information about working time limits.
England
- Care Quality Commission (CQC) monitors, inspects and regulates services to ensure standards of safety and quality.
- CQC and Ofsted jointly inspect local areas to assess how they fulfil their responsibilities for children and young people with special educational needs and/or disabilities.
- NHS England National Quality Board – provides guidance on safe, sustainable and productive staffing.
- National Institute for Health and Care Excellence – provides guidance, advice, quality standards and information services for health, public health and social care.
- NHS England Change management resources
Wales
- AcademiWales – learning and development for leaders and managers working across the public service in Wales
- Care Inspectorate Wales – regulates and inspects to improve the quality and safety of services for the well-being of the people of Wales.
- Healthcare Inspectorate Wales (HIW) – independent inspectorate and regulator of healthcare in Wales.
- National Institute for Health and Care Excellence – provides guidance, advice, quality standards and information services for health, public health and social care.
- Improvement Cymru – national improvement service for Wales – part of the Quality, Safety and Improvement directorate of the NHS Wales Executive.
Scotland
- Care Inspectorate (Scotland) – The Care Inspectorate regulates and inspects care services in Scotland to make sure that they meet the right standards.
- Heath Care Improvement Scotland – provides clinical standards, guidelines and advice based upon the best available evidence.
- Health (Tobacco, Nicotine etc. and Care) (Scotland) Act 2016 – imposes a Duty of Candour on all health service staff to report incidents that could bring harm or have brought harm to individuals.
- Scottish Intercollegiate Guidelines Network (SIGN) – SIGN develops evidence-based clinical practice guidelines for the National Health Service (NHS) in Scotland.
- Scottish Patient Safety Programme (SPSP) – SPSP is a unique national initiative that aims to improve the safety and reliability of healthcare and reduce harm, whenever care is delivered.
Northern Ireland
- Care Standards – allows for the regulation of a range of health and social care services, and for the development of minimum standards for these services.
- Education Training Inspectorate – promotes the dissemination of good and innovative practice identified across the education, training and youth sectors.
- National Institute for Health and Care Excellence – provides guidance, advice, quality standards and information services for health, public health and social care.
- Northern Ireland Public Services Ombudsman – provides for an independent review of people’s complaints and ensures that public services improve as a result of the complaints.
- Patient and Client Council – the independent voice for people using health and social care services.
- Quality 2020 – 10 Year strategy designed to protect and improve quality in health and social care in Northern Ireland.
- Regulation and Quality Improvement Authority (RQIA) – responsible for monitoring and inspecting the availability and quality of health and social care services.
- ‘Up to standard’ (PDF) – guide to the Quality Standards for Health and Personal Social Services
Resources
RCSLT Resources
RCSLT has many resources which provide further information to support building a business case:
- Staffing and resourcing – explore how to achieve an efficient and effective service within given resource parameters.
- Quality services
- Collaborative working– information on working collaboratively, including in multidisciplinary teams and cross agency working.
- Local influencing– tips to help demonstrate the benefits of speech and language therapy.
- Clinical guidance topics and settings– find out more about the evidence for individual topics and benefits of speech and language therapy involvement in different settings and clinical areas.
- Care Pathways – this sets out the anticipated course of care towards positive outcomes for an individual within a designated care group; for example, individuals with progressive neurological disorders or school-aged children with a speech, language or communication disorder.
- RCSLT factsheets– A series of factsheets about how speech and language therapy transforms lives in different settings and clinical areas.
- Health inequalities
- Outcome measurement includes information on outcome measurement, choosing an appropriate outcome measure and the RCSLT online outcome tool (ROOT).
- Invest in SLT petition
- Children’s services guidance
External Resources
- NHS overview of demand and capacity planning provides and overview of demand and capacity modelling and how you can use this for planning in the NHS (2023) – Video (plays on YouTube)
- The NHS England Demand and Capacity team has a range of models you can use to help you understand the needs of your service.
- NHS quality improvement and redesign tools stakeholder analysis
- Health Services Management Centre (HSMC) at the University of Birmingham is one of the UK’s foremost centres for research, evaluation, teaching and professional development for health and social care organisations.
- NHS Networks – create and manage a network or community of interest. Take part in discussion forums, share knowledge on good practice, including videos and presentations. Get news, views and information about events.
- NHS set of business planning resources and templates
- What works database from Speech and Language UK
- Equity for All (2022): Children’s Speech and Language Therapy services in Scotland
- The demand and supply of therapists for Children and young people with SEND: a scoping study
- Understanding the Therapy Needs of Children with Complex Needs Across South East England
- Bercow review 10 years on
- Talking about a generation
- Leadership of Allied health professions in trusts what exists and what matters (2018)
- Better Communication – shaping speech, language and communication services for children and young people
- The Balanced System: Better Communication The Balanced System® is an outcomes-based framework and suite of tools and templates that can be used to improve the commissioning and delivery of services for children and young people which benefit from an integrated approach to delivering outcomes.
Contributors
Lead Author
- Maria Luscombe FRSCLT
Supporting Authors
- Jo Bradburn, Deputy Director of Allied Health Professions and Speech and Language Therapist
- Natacha Capener, Lecturer and Speech and Language Therapist
- Nicola Holmes, Chair of ASLTIP
- Wing yee Lam, Practice Development Speech and Language Therapist
- James Martin, Highly Specialist Speech and Language Therapist (Head & Neck)
- Katie Masters, Specialist Speech and Language Therapist
- Claire Matheson, Service Lead Adult Learning Disability
- Rosalind Gray Rogers, Programme Director for Speech and Language Therapy
- Jo Taylor, Speech and Language Therapist
- Paula Walker, Highly Specialist Speech and Language Therapist
