Goal setting – guidance
Information on goal setting guidance for SLTs.
Last updated: April 2026
Back to Delivering quality services
 Download as PDF
Download as PDF- Introduction
- Management phase
- Goal setting principles
- Multidisciplinary goal setting
- Types of goals
- Timing of intervention
- Reflective practice
- Resources
- Contributors
Introduction
Goal setting is core to managing individual care plans.
Speech and language therapists work collaboratively with service users and their key support partners, to identify goals, aims or targets (called goals from now on). Service users and their key support partners should be actively involved in the development, design and evaluation of therapy programmes/interventions. Goals and outcome measures help guide mutually realistic interventions.
The overall management plan and the individual goals should:
- have a timescale
- be drawn up in consultation with the individual where possible and based on outcomes that are important to them
- be a collaboration with the individual and their key support partners, where appropriate
- be shared with the service users, carers or other professionals
- detail aims, objectives, and expectations of intervention/management
- relate to the individual’s communication or eating/drinking needs, activity, participation, and wellbeing
- be realistic, regularly reviewed, reflected on, and adjusted as required
- be ethical
- be relevant to the individual, carers, and context
- be needs based
- be evidence based (where evidence is available)
- focused on functional, participative aspects of life wherever possible.
Goals should be defined in agreed terms, i.e. using shared terminology and jargon free.
Management phase
Purpose of management
To implement an appropriate, timely and integrated approach to the management of the individual’s difficulties involving the individual, the family, other professionals and key people in the individual’s environment.
Intervention may be in English, in another language, bilingual or carried out through an interpreting service. A judgement of what is appropriate will be based on individual circumstances, evidence-based guidance, where available, and professional consensus opinion on what is appropriate for particular conditions and settings.
SLTs should be aware of any national service pathways that apply to their care group and how this might impact on an individual’s care plan.
Principles underpinning management of referred individuals
- Intervention is informed by the best available evidence and underpinned by the consent of the individual and/or carer
- Speech and language therapy works to encourage individual autonomy and to discourage dependency on the therapist, thereby enabling individuals to take an active role in managing their condition wherever possible
- Speech and language therapy works to reduce the health, educational and psychosocial risks faced by the individual
- Speech and language therapy works to promote individual access to and participation in everyday life activities
- Person-centred intervention is based on an holistic understanding of the individual and all aspects of their life
- Intervention should be based on individual need and should take account of available evidence and consensus guidance on effective practice. Intervention should promote individual safety and that of carers and staff
- An intervention plan is likely to include work to change or maintain the individual’s functional ability as well as work to address the impact of their condition when participating in community life
- Speech and language therapy intervention aims to be efficient as well as effective
- Continuity of care is an important aspect of effective practice. Intervention will take full account of the individual’s preferred language, culture, lifestyle and environment, including the role that carers can play
- Whenever appropriate, intervention should be provided as part of a multi-agency team. Where there is a choice, intervention should be provided in the most conducive setting for optimising effectiveness
- The most effective approach for working with individuals involves integrated and coordinated working across community and acute settings
- The service considers RCSLT guidance on working relationships between independent and public sectors
- Intervention should be matched to the needs, strengths and capacities of each individual and modified as these change over time
- Communication and eating/drinking are fundamental rights, meaning that SLTs should ensure that such disorders do not preclude opportunities for self-determination, fulfilment and participation in community life
- Intervention aims to make communication and eating/drinking as positive an experience as possible
- Speech and language therapy values and incorporates all means of communication within intervention planning
See also:
Planning options
A management plan should be established in conjunction with the individual and/or key people in the their life, whenever possible and appropriate.
Physical and/or sensory impairment should not restrict consideration of augmentative and alternative communication (AAC), given the advances in technology; however, in some cases such disability may be a significant barrier.
An individual, their family, and the team should be provided with all relevant and necessary information pertaining to the rationale behind the intervention programmes, in order to make informed decisions regarding their care.
Written consent should be obtained when intervention involves:
- Heightened levels of risk (for example, invasive procedures)
- Participating in teaching or research projects
- Photographic or audio-visual recordings of the individual
- Where a client is unable to give consent, this should be sought from legally authorised parties.
All written and spoken information should be clear and accessible to the recipients.
To include carers whose preferred language is not English, the services of an appropriately bilingual therapist or SLT co-worker may be required. Where this is not possible, interpreting and translation services should be used. This will require time in the session for briefing and de-briefing the interpreter.
Where the care is provided as part of a multi-professional approach, management plans may also be multidisciplinary. Where many professionals are involved with an individual, one named person will take the role of coordinating the assessment and management amongst a large and sometimes geographically fragmented group. In this situation, speech and language therapy should be provided, in conjunction with the key support person.
If appropriate and agreed with the individual, the speech and language therapy management plan will be shared with members of the multi-professional team. The management plan will take account of the individual’s environment and priorities and, in the case of children, the priorities of the carer and will be made available to the client within two weeks of the completion of the assessment process.
Setting aims as part of the management process
Goals should derive from a consideration of the individual’s needs and wishes as well as the therapist’s opinion based on comprehensive assessment and reference to the evidence base.
Therapists will advise on what is likely to be achievable in the short and long-term, taking all the relevant factors into account. This may involve:
- resolving a particular aspect of communicative/swallowing function, achieving optimal improvement of function (as estimated by taking all factors into account)
- maintaining optimal function, for example, through the use of compensatory strategies
- enabling increased independence through making changes within the individual’s environment
- avoiding the development of secondary difficulties.
In support of this, the therapist may, with the individual, plan to work on one or more of the following goals to:
- enable the individual/carer to access relevant systems/services/learning environment
- optimise participation in educational, social, work and recreational activities, as appropriate
- inform others about the nature of the communication or eating/drinking need and the process of intervention
- advise and assist the individual/others in the use of facilitative strategies
- help maximise the individual’s communication/eating and drinking skill development
- Recommend an AAC system as appropriate, and enable its use
- train others in the use of supportive strategies or teaching tasks
- provide information for individual/carer on the possibility of further difficulties
- find ways of preventing the development of further difficulties
- advise on risk-reduction
- support the individual/carer in coping optimally with the present condition
- help the individual/carer come to terms with difficulties
- implement an agreed programme of therapy/intervention, whether directly or indirectly; through training and advising other agents to conduct a specific programme (which an SLT will monitor and adjust as necessary)
- continue to discuss ultimate (long-term) goal and discharge criteria.
Where appropriate, for example, in the context of a deteriorating condition, the following aims may apply:
- to work with and through others, in support of the individual in order to maintain stability and prevent deterioration for as long as possible
- advise on risk-reduction
- provide the individual with strategies to maintain stability
- support the individual and carers in coping with a sudden or a slowly deteriorating condition
- to provide physical, psychological and social support as part of the team.
Goal setting principles
Goals may relate to behaviour; skills; knowledge; attitudes; values; emotional state, and medical condition of the referred individual. Goals may also relate to the behaviour, skills and attitudes of those within the individual’s environment.
It is recommended that goals are:
- ethical
- relevant to the client, carers and context
- needs-based
- evidence-based (where evidence is available)
- focused on functional, participative aspects of life wherever possible
- formulated in conjunction with client/carer
- formulated in conjunction with other members of the team, where appropriate
- specific, measurable, achievable, relevant, and timed (SMART, SMARTER)
- defined in agreed terms, i.e. using shared terminology. This may involve using the client’s opinion, in words or in another form of communication.
- jargon-free
- take into account the skills and knowledge of the agent of change
- regularly reviewed
- discussed, agreed and evaluated with clients and, where appropriate, with carers.
Common frameworks used for setting goals include:
- SMART – specific, measurable, achievable, realistic, timely
- SMARTER – shared, monitored, accessible, relevant, transparent, evolving, relationship-centred
- Frameworks, such as Goal Attainment Scaling (GAS) can be used to score the extent to which individual goals are attained over the course of therapy.
Goal setting should be subject to periodic peer-review. It should be noted that, because of the subjectivity and variability around goal setting, goal-achievement data cannot be aggregated and used as a benchmark for services.
Multidisciplinary goal setting
Within all agencies in the UK, there is an increasing emphasis on multidisciplinary working and joint goal setting. Although goals in certain settings (for example, independent practice), or for certain individuals (for example, adults with dysfluent speech, or preschool children who are not accessing daycare), may be uni-disciplinary, therapists may often need to link with other agencies or professions in setting goals.
There is currently no law covering joint team accountability. This means that each professional carries individual accountability for their actions carried out (or not carried out) within the team. Where joint working is undertaken and where appropriate, any speech and language therapy-specific outcomes should link to those of other professionals. Respective roles and contributions of personnel should be specified when achieving outcomes is dependent on other professionals.
Types of goals
The World Health Organisation’s International Classification of functioning disability and health, provides a useful framework for considering goal type.
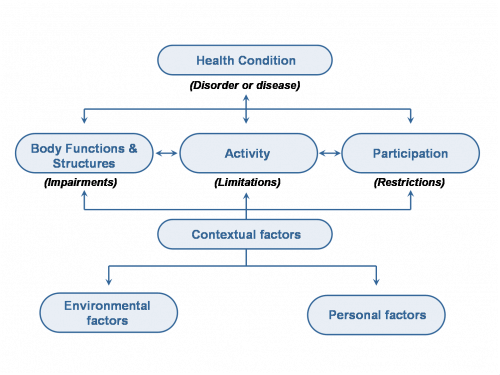
Goals that impact on change for the individual may be developed for:
- the individual
- their key communication partner
- their immediate social network
- their community.
The goals may target:
- impairment
- access to activity
- barriers to participation
- social and environmental barriers
- health and wellbeing.
Models of delivery include:
- individual input: direct or indirect, (i.e. working with and through others)
- group therapy
- review appointments for advice, support and monitoring. This may be in the context of specialist clinics or support groups
- joint sessions with other professionals/workers
- carer education and training
- consultation/liaison services
- carer support groups
- workshops and training sessions for people who may then act as agents of change.
Goal types include:
- reducing needs or barriers
- teaching strategies
- conversational skills
- self-advocacy
- personal portfolios
- counselling
- enhancing communication
- provision of accessible information
- use of technology
- conversational partner training
- environmental modifications.
Intervention may involve giving advice, making recommendations, leading therapy activities, as well as providing support and education for the individual, their family, carers, and the multidisciplinary team.
Carers may be the legitimate focus of intervention. Review and discharge procedures should be discussed as part of the management plan. The agreed plan of action should be made clear within the case notes, dated and signed.
Timing of intervention
Timing of intervention should be determined by an evaluation of the individual’s readiness and ability to change (or the potential to change the environment). This should also take into account the individual’s motivation to change, and the level of support available.
Rationale
An individual’s ability to respond to therapy can be affected by many factors, both internal and external, and it is important to give consideration to these during the period of care.
Evidence
For evidence relating to specific client groups and settings see individual topics in our clinical guidance A to Z.
Reflective practice
It is recommended that management aims and objectives are reviewed regularly and frequently. If anticipated progress is not achieved, the therapeutic intervention should be reviewed.
Clinical supervision aids reflective practice.
Resources
- RCSLT professional development scenario – goal setting for groups
- RCSLT professional development scenario – auditing therapy goals and outcomes
- King’s College Hospital – Goal Attainment Scaling information and downloads
- Shared decision making within goal setting in rehabilitation settings: A systematic review. Patient Education and counselling 100(1), 65-75 – a systematic search of databases on this topic between 2005 and 2015
- Taliancich-Klinger, C., Kennedy, A. J., & Eaton, C. T. (2025). Goal setting in speech-language pathology : a guide to clinical reasoning (1st ed.). Plural Publishing Inc.
- Ørjasæter, K. B., & Mueser, K. T. (2023). Meaningful Goal Setting: Practitioners’ Perspectives on Goal Setting in the Illness Management and Recovery Program. Psychiatric Rehabilitation Journal, 46(1), 94–100. https://doi.org/10.1037/prj0000564https://doi.org/10.1037/prj0000564
- Van de Velde, D., Boeykens, D., Gauwe, V., Steyaert, G., Ryssen, L., Jarrey, M., Boeckxstaens, P., Pype, P., & De Vriendt, P. (2025). Goals should be defined as CLEVER before specifying them into SMART goals: A phenomenological hermeneutical study to facilitate the implementation of goal-oriented care in primary care. The British Journal of Occupational Therapy. https://doi.org/10.1177/03080226241311683https://doi.org/10.1177/03080226241311683
- Are SMART targets smart or stupid? EQUALS
- Okita, Y., Kawaguchi, Y., Inoue, Y., Ohno, K., Sawada, T., Levack, W., & Tomori, K. (2024). Characteristics of goal-setting tools in adult rehabilitation: A scoping review. Clinical Rehabilitation, 38(2), 234–250. https://doi.org/10.1177/02692155231197383https://doi.org/10.1177/02692155231197383
- Lawton, M., Sage, K., Haddock, G., Conroy, P., & Serrant, L. (2018). Speech and language therapists’ perspectives of therapeutic alliance construction and maintenance in aphasia rehabilitation post‐stroke. International Journal of Language & Communication Disorders, 53(3), 550–563. https://doi.org/10.1111/1460-6984.12368https://doi.org/10.1111/1460-6984.12368
RCSLT members can access journal articles via our journals collection A to Z.
Contributors
Kathryn Cann
Natacha Capener, Lecturer and Speech and Language Therapist (2025 update)
